
































































































In most medical professions, we tend to put different parts of the human condition into neat little boxes.
As a hand therapist, early on in my career I tried just to treat hands, wrists and elbows with the occasional shoulder thrown in when warranted.
The problem was, I often times would feel like Bugs Bunny trying to stop leaks in a dam. Every time I would solve one problem, another would pop up further up the arm or another part of the hand.
I kept trying to find the "right" exercise or the "right" intervention. When I felt like I found the appropriate exercise or intervention I wanted to know what the "right" number of sets or repetitions was.
I wanted to be able to give my patients the answer. I wanted to "fix" their particular diagnosis. In school, this was taught as a "Biomechanical Frame of Reference".
For years, I thought this was the only framework in which I needed to operate. But the human body is not just a system of made of muscles and bones strapped together with ligaments and connective tissues.
There's a vast network of nerves that courses throughout nearly every inch of our body acting as a two-way electrical system, sending signals to and from all of these mechanical structures. And all of this influences and is influenced by our endocrine system, which release all sorts of hormones and chemicals that can change the very physiology of our body.
All of this is why I now try to think of recovery from injury, be it chronic repetitive strain or acute, from three different frames of reference: Bio-mechanic, Neuromuscular, and Psychosocial.
Let's dig into that with an example.
Imagine there are two people undergoing the exact same surgery for trigger finger, which is a fairly straight forward surgery for a condition that occurs in roughly 2-3% of the population.
One patient is a 27-year-old woman who has a decent paying job, recently married but without children who started having symptoms about a month after she started trying rock climbing in her spare time.
The other patient in a 63-year-old male who has had symptoms for the last 2+ years but he couldn't afford to take time away from his job as a mechanic. In addition to his regular job, he has been helping his daughter by giving regular childcare to his grandkids. The only reason he can make time to have surgery now is that he was recently caught up in a round of layoffs.
From a Biomechanical perspective, I would treat these two people the exact same way.
But the 62-year-old has higher than expected pain because he can't stop picking up his 2-year-old grandson to change his diaper, so I need to treat the irritated nerve and the high pain response and most likely I need to retrain him to move in a less guarded fashion during functional activities. This would be a more Neuromuscular approach.
And finally, I imagine that part of the reason his pain is high and his movement patterns are dysfunctional, is that his stress level is through the roof.
So I need to problem solve ways with him that he can adapt his functional activities to create less stress on his healing tissue. I might even talk about things like diaphragmatic breathing and controlled loading with exercise to reduce stress and thereby reduce cortisol and adrenaline levels.
And before I can introduce these ideas, I have to get him to trust me enough to get past the idea that his finger will eventually get better with some splinting and finger exercises. This is a Psychosocial approach.
These ideals can be incorporated into joint support design as well. Most over-the-counter splints and braces I have seen used in my career are very functional and very "medical looking". That's because they are usually designed with a functional Biomechanical approach.
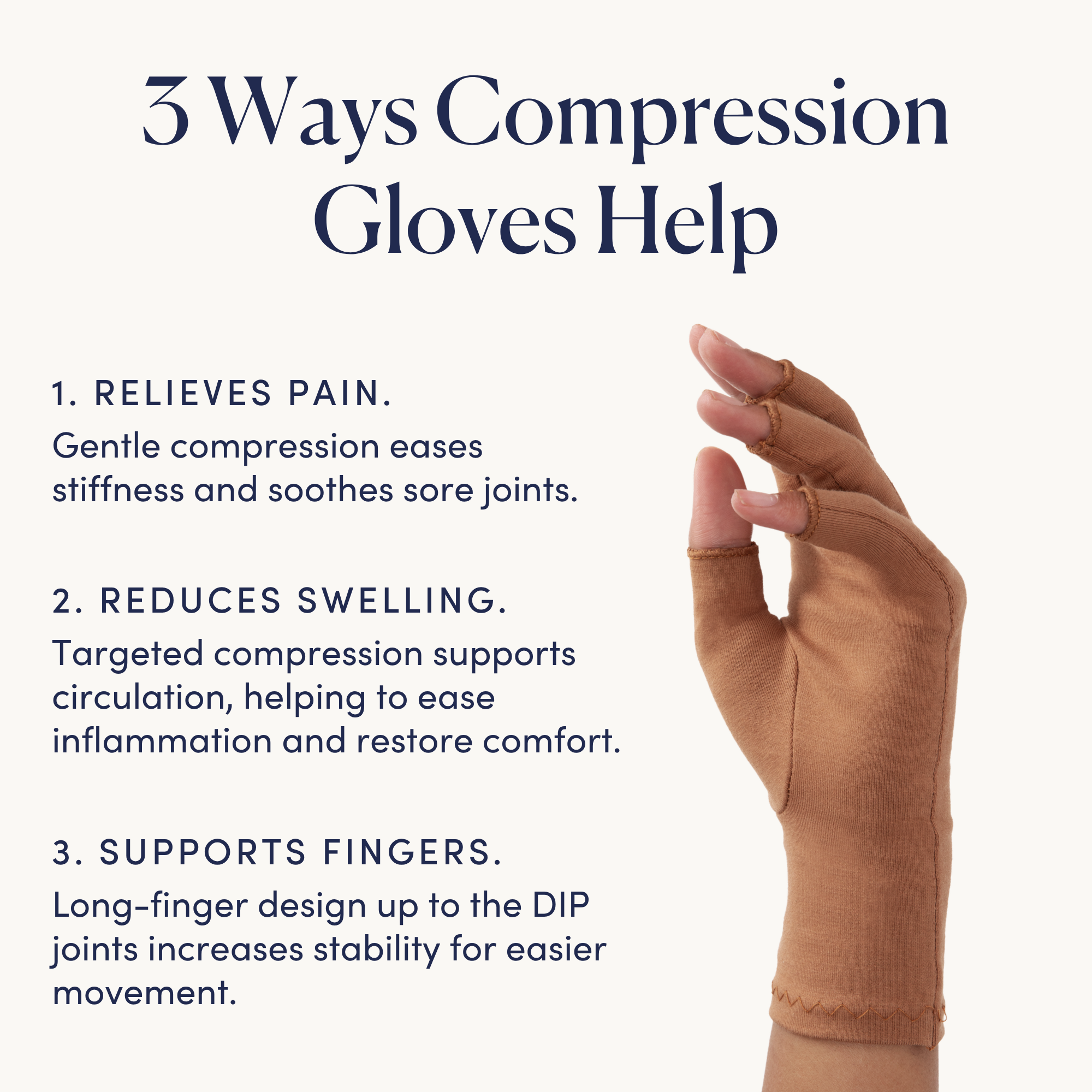
But a good splint or support shouldn't just hold a wrist and hand in a safe position for healing. It should incorporate the above therapeutic approaches. It should provide comfort and compression in key areas to calm irritated nerves and chronically painful structures.
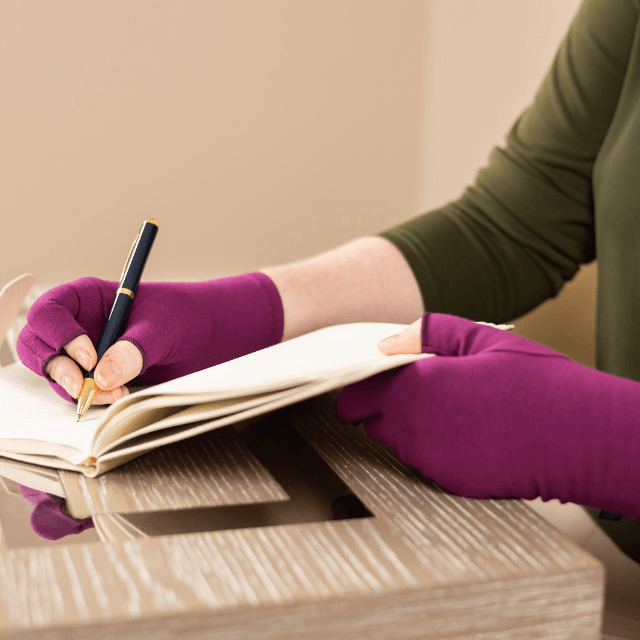
And it should also have a stylish and comforting aesthetic, so someone doesn't have to grimace as they prepare for a day filled with people asking "What did you do to your arm!?" as they go about their business with a clunky medical device strapped to their wrist.
This is our goal with Grace & Able. To design joint support that supports the whole person and not just the wrist.
Trevor Petrie, Certified Hand Therapist
Trevor Petrie is a Certified Hand Therapist with a Master’s degree in Occupational Therapy from the University of Washington.
He has been helping people with hand and upper extremity pain and injuries since 2012.
Over the course of his career, he has treated hundreds of people with chronic pain stemming from a myriad of causes including osteoarthritis, rheumatoid arthritis, carpal tunnel and tendinitis.
No two people experience these issues the exact same way, so Trevor strives to find the best evidence-based approach that works for each person’s individual needs in order to get back to living their best lives.


Share and get 15% off!
Simply share this product on one of the following social networks and you will unlock 15% off!